Most parent and people have at one point in time experienced a child having a seizure and completely do not know what to do, or sometimes end up doing something that might cause more harm for the seizing child. Watching a child experience a seizure is a profound and often distressing event for parents, so today we are going to discuss seizures in children and what should and should not be done, so let’s go ahead and understand what seizures really are.

Throughout Africa , these episodes are recognized by various traditional names that reflect localized cultural understandings. For example, in East Africa, the Swahili term Kifafa is widely used, while in Uganda, it is known as Ensimbu among the Luganda. In Southern Africa, the Zulu refer to it as Isithuthwane, and in Zimbabwe, the Shona people may use terms like Pfari (referring to jerking) or Tsviyo. In West Africa, names include Adingbe (Fon, Benin), Wayoo (Mandinka, The Gambia), and the Yoruba term Warapa. While the immediate priority is always safety, understanding the why this is happening and the specific types of pediatric seizures is important as this helps carer’s composure and actions. A seizure is an episode of altered behavior, movement, or consciousness caused by sudden, abnormal electrical activity in the brain (in other words, the brain is misfiring). This electrical surge disrupts the normal communication pathways between neurons, leading to physical manifestations that range from subtle staring spells to vigorous muscle contractions (AKA Convulsion).
Understanding the different Types of seizures in Children
Seizures are not a singular condition but rather a symptom of various underlying neurological processes. Clinicians typically categorize them into two broad groups based on where the electrical activity begins.
- Focal Seizures: Formerly known as partial seizures, these originate in one specific area or hemisphere of the brain. They may present as twitching, unusual sensory changes, or repetitive movements of only one particular area of the body .
- Generalized Seizures: These involve both sides of the brain from the onset and usually result in a loss of consciousness. They are further divided into specific subtypes based on physical symptoms, but for simple understanding it affect almost all part of the body at once. The two most common types are given as examples below
- Tonic-Clonic Seizures: Perhaps the most recognized type, these involve a phase of muscle stiffening (tonic) followed by rhythmic jerking (clonic), you typically see the child shaking the hands and feet violently in up and down motion.
- Absence Seizures: These are subtle and often mistaken for daydreaming or lack of attention, as the child briefly loses awareness without falling or shaking.

According to the Epilepsy Foundation (2025), identifying the specific seizure type is essential for determining the appropriate long-term treatment and prognosis.
Common Causes of Pediatric Seizures
While the specific cause of a seizure can sometimes remain idiopathic (unknown), medical evaluations typically focus on a few primary triggers. In pediatric patients, the developing brain is often more sensitive to physiological changes and external stressors than an adult brain. Here are common causes of seizures in children
- Fever (Febrile Seizures): The most common type, which occurs in approximately 2% to 5% of children between the ages of six months and five years, usually due to a common viral infection rather than a disorder of the brain itself. The seizure is usually triggered by the pace of the temperature change rather than the high degree of the fever itself. Most febrile seizures are “simple,” meaning they last less than fifteen minutes and do not recur within a 24 hour period. Research from the National Institute of Neurological Disorders and Stroke (2024) indicates that while these events are terrifying for parents, simple febrile seizures do not cause brain damage or typically lead to epilepsy in later life.
- Genetic Factors: Some children inherit a lower seizure threshold from their parents. Various genetic syndromes are linked to epilepsy, where specific gene mutations affect how ions flow in and out of brain cells.
- Head Trauma: Significant injuries to the brain, such as those from a fall, car accident, or sports injury, can cause immediate seizures or create scar tissue that leads to seizures later in life.
- Infections of the Central Nervous System: Conditions like meningitis or encephalitis which involve inflammation of the protective membranes or the brain tissue itself can trigger acute seizures.
- Prenatal or Developmental Issues: Brain malformations that occur during pregnancy, or oxygen deprivation during birth (hypoxic-ischemic encephalopathy), can result in neurological irritability.
- Metabolic and Chemical Imbalances: The brain requires a delicate balance of chemicals to function. Significant drops in blood sugar (hypoglycemia) or imbalances in electrolytes like sodium, calcium, or magnesium can trigger an episode.
- Ingestion of Toxins: Accidental ingestion of certain medications, lead, or other poisonous substances can lead to seizure activity in curious toddlers.
We now know how the different types of seizures look like and there possible causes, let now find out what to do when a child develops one.
Immediate Response Protocol
When you notice a child is having a seizure, the primary goal is to prevent injury. Most seizures are self limiting and will resolve on their own within a few minutes. Adhering to a standardized safety protocol ensures the child remains protected until the episode passes.
- Keep your composure and track the time. Knowing the exact duration of the seizure is vital for medical assessment.
- Clear the immediate area of hard or sharp objects. If the child is on the floor, move furniture away to prevent impact injuries.
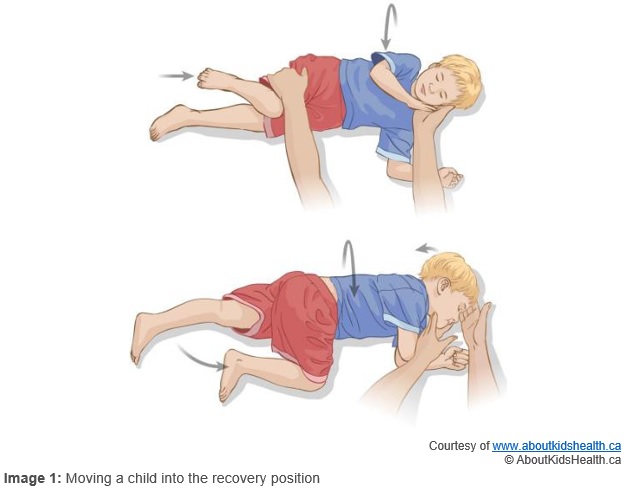
- Ease the child onto the ground and place them on their side. This “recovery position” helps keep the airway clear and allows saliva or vomit to drain out of the mouth, preventing aspiration.
- Cushion the child’s head. Use a folded jacket or a small pillow to protect the skull from repetitive contact with the floor.
- Loosen restrictive clothing. Undo buttons or ties around the neck to ensure breathing remains unobstructed.
Critical things to avoid doing during a seizure
Misconceptions about seizure first aid can lead to dangerous interventions. It is vital to avoid certain actions that could inadvertently harm the child.
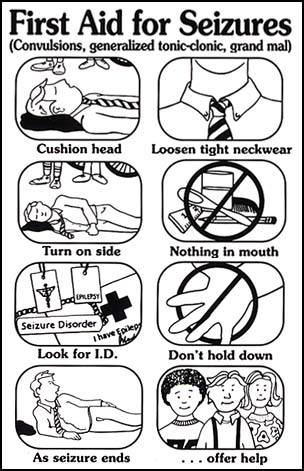
- Do not restrain the child. Forcing a child to stop moving during a seizure can result in bone fractures or muscle tears.
- Never place anything in the child’s mouth especially spoons, herbs, oil . There is a persistent myth that a person can swallow their tongue during a seizure; this is physically impossible. Placing objects like spoons or fingers in the mouth can lead to broken teeth or bitten fingers.
- Avoid mouth to mouth resuscitation. Children may breathe irregularly or appear dusky during a seizure, but they usually resume normal breathing once the episode ends.
- Do not offer food, water, or medication until the child is fully conscious and alert. Giving fluids to a drowsy child can lead to choking.
- Do not place their feet’s close to or inside a fire, as this is of no use and will lead to them having degree burns
When to Seek Emergency Medical Attention
While many seizures do not require an emergency room visit, certain “red flag” situations necessitate immediate intervention via emergency services. You should call for an ambulance if the seizure lasts longer than five minutes, which may indicate a state of status epilepticus, a prolonged seizure that requires intravenous medication to stop. Other reasons for emergency care include the child having difficulty breathing after the seizure, the occurrence of a second seizure immediately following the first, or if the seizure happens in water. The Mayo Clinic (2025) notes that a first time seizure always requires an urgent medical evaluation to rule out underlying causes like meningitis or electrolyte imbalances.
What to expect after the siezure
The period immediately following a seizure is known as the postictal phase. During this time, the brain is recovering, and the child may feel exhausted, confused, or irritable. They may sleep deeply for several hours. Once the child is stable, a pediatrician or pediatric neurologist will likely perform a series of diagnostic tests.

The diagnostic process often includes an electroencephalogram (EEG), which records the electrical activity of the brain to look for patterns associated with epilepsy. In some cases, neuroimaging such as a Magnetic Resonance Imaging (MRI) scan is used to ensure there are no structural abnormalities.
Frequently Asked Questions
Can a fever cause a permanent brain injury during a febrile seizure?
Current medical data from the American Academy of Pediatrics (2025) confirms that simple febrile seizures are benign. They do not affect a child’s intelligence, academic performance, or long term neurological health.
What is the difference between a seizure and epilepsy?
A seizure is a single event. Epilepsy is a chronic condition characterized by two or more unprovoked seizures. Not every child who has a seizure will develop epilepsy.
Should I give my child fever reducing medication to prevent a seizure?
While acetaminophen or ibuprofen can make a child more comfortable during an illness, studies show that these medications do not necessarily prevent a febrile seizure from occurring, as the seizure is often triggered by the rate of temperature rise rather than the peak temperature itself.
How long does the recovery phase usually last?
The postictal state varies. Some children bounce back within ten minutes, while others may remain groggy or have a headache for several hours.