
Breast cancer has emerged as the most common malignancy and the leading cause of cancer-related death among women in sub-Saharan Africa. While historically incidence rates were lower than in Western nations, the mortality burden is disproportionately severe.
Rising Incidence, High Mortality
Global data show that in 2022 there were 2.3 million new cases of breast cancer and more than 666,000 deaths worldwide. In the African region, the burden remains substantial: in sub-Saharan Africa (SSA) alone, a large proportion of global breast cancer deaths occur.
According to a 2018 GLOBOCAN estimate, Africa recorded around 168,690 new breast cancer cases and 74,072 deaths in that year. The age-standardized incidence rate across the continent stood at approximately 37.9 per 100,000 women, with wide variation between countries (as low as 6.9/100,000 in The Gambia, and as high as 69.6/100,000 in Mauritius).
A recent assessment by the World Health Organization (WHO) for its African Region reported that sub-Saharan Africa is expected to experience nearly double the number of new breast cancer cases by 2040 if current trends continue. Sad right?
Despite an increase in cases, mortality remains disproportionately high. In many African settings, five-year survival rates remain below 50 percent. This contrasts sharply with outcomes in high-income countries, where five-year survival often exceeds 90 percent when cancers are detected early.
The Biological Landscape: Types and Distinct Patterns
Here are the main types of breast cancer
Invasive ductal carcinoma (IDC)
The most common type. It starts in the milk ducts and then spreads into surrounding breast tissue. IDC can spread to lymph nodes if not detected early.
Invasive lobular carcinoma (ILC)
Begins in the milk-producing lobules. It often grows in a subtle pattern, which can make it harder to detect on imaging.
Ductal carcinoma in situ (DCIS)
A non-invasive form where abnormal cells remain inside the ducts. It is highly treatable because it has not spread beyond the duct.
Lobular carcinoma in situ (LCIS)
Not a true cancer but a marker of increased future risk. Abnormal cells are found in lobules, and women with LCIS need regular monitoring.
Triple-negative breast cancer (TNBC)
Lacks estrogen receptors, progesterone receptors and HER2. It grows quickly, is more common in younger African women, and often requires chemotherapy.
HER2-positive breast cancer
Tumours overexpress the HER2 protein, making them aggressive. They respond well to targeted therapies such as trastuzumab when available.
Inflammatory breast cancer (IBC)
A rare but fast-growing type. It causes redness, swelling and skin changes instead of a traditional lump. IBC often presents at an advanced stage.
Paget disease of the breast
A rare cancer that affects the nipple and areola, often presenting with itching, flaking or discharge.
Risk factors for Breast cancer
1. Age: Risk increases as women get older. Most cases occur after age 40, although many African countries see rising cases in younger women.
2. Family history and genetics: Having a close relative with breast cancer raises risk. Mutations such as BRCA1 and BRCA2 greatly increase lifetime risk and often lead to more aggressive tumours.
3. Reproductive and hormonal factors: Early menstruation, late menopause, fewer pregnancies, delayed first childbirth, and shorter breastfeeding duration increase lifetime exposure to estrogen, which raises risk.
4. Lifestyle factors: Obesity after menopause, physical inactivity, alcohol use, and diets high in processed foods contribute to higher risk. Regular exercise lowers risk.
5. Previous breast disease: A history of atypical hyperplasia or previous breast cancer increases the chance of developing another tumour.
6. Radiation exposure: Past chest radiation, especially during adolescence for medical treatment, increases long-term risk.
7. Breast density: Dense breast tissue makes cancers harder to detect and is linked to a higher baseline risk.
What to Look Out For: Signs and Symptoms
Early-stage breast cancer is usually painless. The dangerous myth that “if it doesn’t hurt, it’s not cancer” leads many women to ignore painless masses until the disease advances.

Both patients and providers must be vigilant for:
- The Lump: A hard, painless mass in the breast or axilla (armpit).
- Skin Changes: Dimpling (peau d’orange), puckering, or redness.
- Nipple Changes: Retraction (turning inward), spontaneous bloody or clear discharge, or scaling.
- Asymmetry: A sudden change in size or shape of one breast.
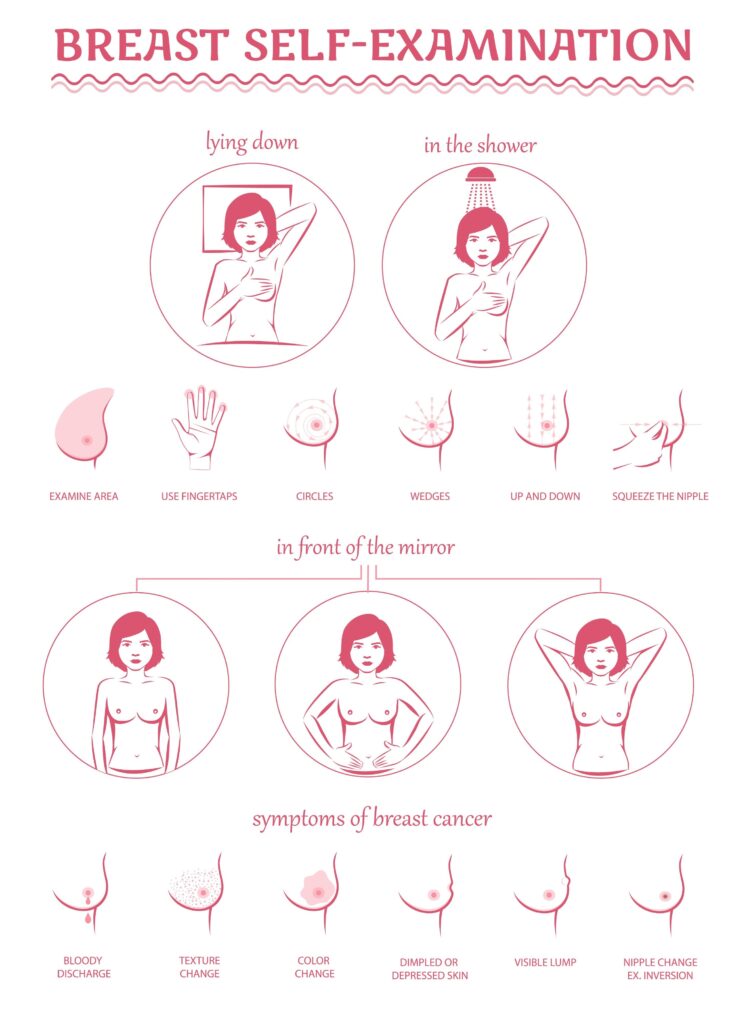
The Vital Role of Breast Self-Examination (BSE)
With mammography screening limited by cost in many regions, “breast awareness” is the primary line of defense.
- When: Monthly, check 3–5 days after the period ends.
- How: Visual inspection in a mirror (arms up, then on hips) followed by manual palpation lying down.
- Technique: Use the pads of the three middle fingers in a circular pattern, checking the entire breast, collarbone area, and armpit.
When to See a Doctor
Immediate referral is required for any lump, nipple inversion, or spontaneous discharge. A common delay factor is the use of traditional remedies; however, cancer is a biological condition that requires medical intervention.
Early Detection: The Prognosis Changer
The stage at diagnosis is the strongest predictor of survival. Currently, 60–80% of patients in sub-Saharan Africa present with Stage III or IV disease, compared to less than 10% in the US.
- Early Stage (I & II): Localized to the breast. Survival rates can exceed 80% with treatment.
- Late Stage (III & IV): Spread to lymph nodes or distant organs (metastasis). In resource-limited settings, survival rates for Stage IV disease are critically low, often below 20%.
Shifting diagnosis from Stage III/IV to Stage I/II is the single most effective way to reduce the mortality rate reported by the Lancet Oncology Commission.
Treatment Modalities
- Surgery: Mastectomy remains common due to large tumor sizes at presentation.
- Systemic Therapy: Chemotherapy is essential for the high prevalence of TNBC. Tamoxifen is crucial for hormone-positive cases.
- Radiotherapy: Access varies by region but is critical for reducing recurrence after surgery.
Frequently Asked Questions (FAQ)
Q: Does a biopsy cause cancer to spread? A: No. A needle biopsy is the only way to confirm diagnosis. It does not cause spread; the delay in getting a biopsy allows the cancer to grow.
Q: Is breast cancer a spiritual attack? A: No. It is a genetic and biological disease. Faith should support, not replace, medical treatment.
Q: Can men get breast cancer? A: Yes. Though rare (<1% of cases), men should report lumps immediately.
Q: If I have no family history, am I safe? A: No. Most women diagnosed have no family history. Being female and aging are the biggest risk factors.
** This Article has been Reviewed by Dr. Chimaobi Felix, MBBS
⚕ Medical Disclaimer
This article is for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before making any health decisions. The Healthy African is not liable for any actions taken based on the information provided on this site.