Lassa fever remains a persistent public health challenge in West Africa, with Nigeria bearing the highest burden of the disease. As an acute viral haemorrhagic fever (VHF) caused by the Lassa virus, it accounts for substantial morbidity and mortality annually.
What is Lassa Fever?
Lassa fever is a zoonotic disease, meaning it is transmitted from animals to humans. The virus is a member of the Arenaviridae family. Its primary host is the “multimammate rat” (Mastomys natalensis), a rodent common in West African households. Unlike many other viruses that kill their hosts, these rats can carry the virus for life and shed it in their urine and faeces without falling ill themselves.

First identified in 1969 in the town of Lassa, Borno State, Nigeria, the disease has since become endemic in several countries, including Ghana, Guinea, Liberia, and Sierra Leone. While many cases remain asymptomatic or mild, the virus can lead to severe multi-organ failure and haemorrhage in approximately 20% of infected individuals (WHO, 2024; Lassa fever – WHO).
2026 Situation Update: What We Know
As of early 2026, Nigeria continues to face seasonal outbreaks, typically peaking during the dry season between November and May. According to recent NCDC data, the first week of 2026 saw 21 laboratory-confirmed cases and 9 deaths across three states: Bauchi, Ondo, and Edo. These three states historically account for the majority of the country’s burden.
A notable concern in the current data is the Case Fatality Rate (CFR), which was recorded at 42.9% in the opening week of the year a sharp rise compared to the same period in 2025 (NCDC, 2026; Premium Times – NCDC Report). This high fatality rate is often attributed to late presentation at treatment centres and low indices of suspicion among healthcare providers. Research into a vaccine is ongoing, with Phase 2 clinical trials currently underway in Nigeria and other West African nations, led by the Coalition for Epidemic Preparedness Innovations (CEPI).
Modes of Transmission and Contact
Understanding how the virus spreads is critical for both community prevention and hospital safety.
- Zoonotic (Rodent-to-Human): This is the most common route. Humans become infected through direct contact with the urine, faeces, or saliva of infected rats. This often happens when food or water is contaminated in the home, or through “aerosolization” inhaling tiny particles of dried rodent excreta while sweeping.
- Human-to-Human: The virus spreads through direct contact with the blood, urine, faeces, or other bodily secretions of an infected person. This is especially dangerous in healthcare settings where Infection Prevention and Control (IPC) measures are inadequate.
- Laboratory Transmission: Accidental exposure can occur during the handling of patient samples if strict biosafety protocols are not followed.
It is important to note that Lassa fever is not spread through casual contact like hugging or shaking hands, provided there is no exposure to bodily fluids (CDC, 2025; About Lassa Fever – CDC).
Signs and Symptoms
The incubation period for Lassa fever ranges from 2 to 21 days. Because the early symptoms are non-specific, it is frequently misdiagnosed as malaria or typhoid fever.
Early Stage (Mild)
Approximately 80% of cases are mild or asymptomatic. Symptoms include:
- Low-grade fever and shivering
- General body weakness (malaise)
- Headache
- Sore throat and muscle pain
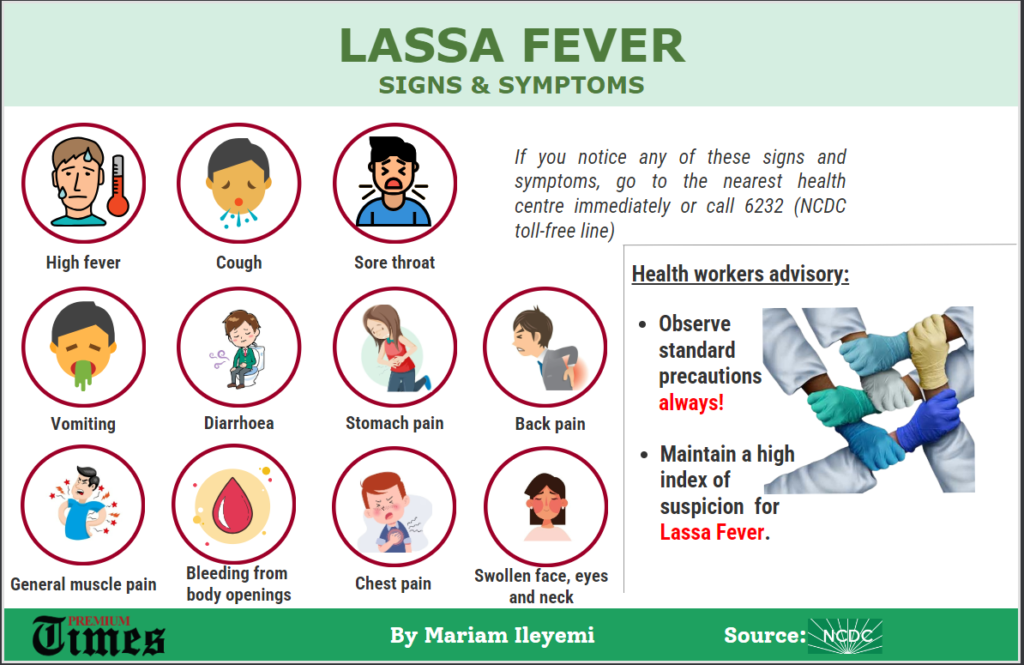
Advanced Stage (Severe)
In the remaining 20% of cases, the disease progresses to involve multiple organs:
- Gastrointestinal: Persistent vomiting, diarrhoea, and abdominal pain.
- Respiratory: Chest pain, cough, and respiratory distress.
- Neurological: Seizures, tremors, disorientation, and coma.
- Haemorrhagic: Bleeding from the mouth, nose, vagina, or gastrointestinal tract.
- Facial Swelling: A common indicator of severe disease progression.
A well-known long-term complication is sensorineural hearing loss, which occurs in about 25% of survivors. In many cases, this deafness is permanent (WHO, 2024).
Protocol of Care and Management
Early diagnosis and treatment are the most effective ways to reduce mortality. Healthcare workers should maintain a high index of suspicion for any patient presenting with a fever that does not respond to standard antimalarial or antibiotic treatment within 48 hours.

- Diagnosis: Gold-standard testing is performed via Reverse Transcriptase Polymerase Chain Reaction (RT-PCR). Other methods include Enzyme-Linked Immunosorbent Assay (ELISA) for antibody detection.
- Isolation: Suspected cases must be immediately isolated in a single-bed room with strict contact and droplet precautions.
- Supportive Care: This includes aggressive fluid management (rehydration), electrolyte correction, and treatment of secondary infections.
- Antiviral Therapy: The drug Ribavirin has traditionally been the standard of care. It is most effective when administered intravenously within the first six days of symptom onset. However, recent reviews by the WHO have called for more robust clinical trials to confirm its efficacy, as some data suggests limited benefits in certain patient groups (WHO, 2025; WHO Ribavirin Review).
- Post-Exposure Prophylaxis (PEP): Healthcare workers with high-risk exposure (e.g., needle-stick injuries) may be considered for a course of oral Ribavirin.
Prevention and Protection
Prevention focuses on “One Health” strategies combining environmental management with personal hygiene.
- Rodent Control: Keep homes clean to discourage rats from entering. Use rat traps and consider keeping cats.
- Food Safety: Store all grains and foodstuffs in rodent-proof containers (plastic or metal with tight lids). Avoid drying food like garri or yam flour in the open air where rats can access them.
- Personal Hygiene: Wash hands frequently with soap and running water. Use alcohol-based hand sanitizers when water is unavailable.
- Safe Burial Practices: The bodies of deceased Lassa fever patients remain infectious. Families should avoid touching the body and instead contact health authorities for safe burial procedures.
For healthcare providers, the use of Personal Protective Equipment (PPE) including gloves, gowns, masks, and eye protection is non-negotiable when dealing with any febrile patient, regardless of the initial diagnosis.
Frequently Asked Questions (FAQ)
Can Lassa fever be cured?
Yes, Lassa fever is treatable, especially if the patient receives medical care and antiviral medication early in the course of the illness.
Is there a vaccine for Lassa fever?
There is currently no licensed vaccine for Lassa fever. However, several candidates are in advanced clinical trials as of 2026.
Can you get Lassa fever from eating rats?
Yes. In some communities where rats are caught and prepared for food, the handling and consumption of these rodents pose a high risk of infection.
Does everyone who gets Lassa fever bleed?
No. Haemorrhaging (bleeding) usually only occurs in severe cases. Most people experience only mild, flu-like symptoms.
How long does the virus stay in the body after recovery?
The virus can persist in the urine for weeks and has been found in the semen of survivors for up to three months. Recovered individuals are advised to practice safe sex during this period.
** This Article has been Reviewed by Dr. Chimaobi Felix, MBBS
⚕ Medical Disclaimer
This article is for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before making any health decisions. The Healthy African is not liable for any actions taken based on the information provided on this site.