Colon cancer, also often included under the umbrella term colorectal cancer (CRC), refers to malignant tumours that arise in the large intestine (colon) or rectum. On the African continent, the disease is emerging as a considerable public health challenge. Here we talked about the latest evidence on what colon/colorectal cancer is, its risk factors, early signs, detection and treatment, and then focuses on the specific drawbacks and barriers in Africa.
What is colon (colorectal) cancer
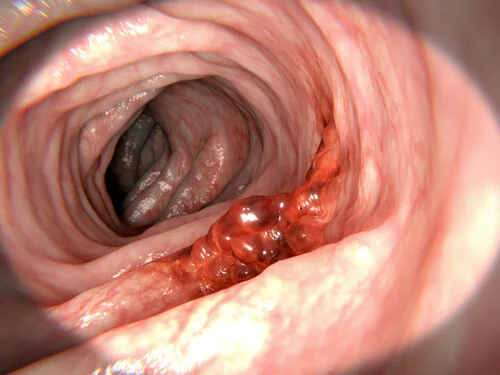
Colon cancer arises when the cells lining the colon or rectum begin to divide abnormally, form a tumour and may eventually invade neighbouring tissues and spread (metastasize) to distant organs. Many colorectal cancers begin as adenomatous polyps—benign growths in the colon lining that over time may become malignant.
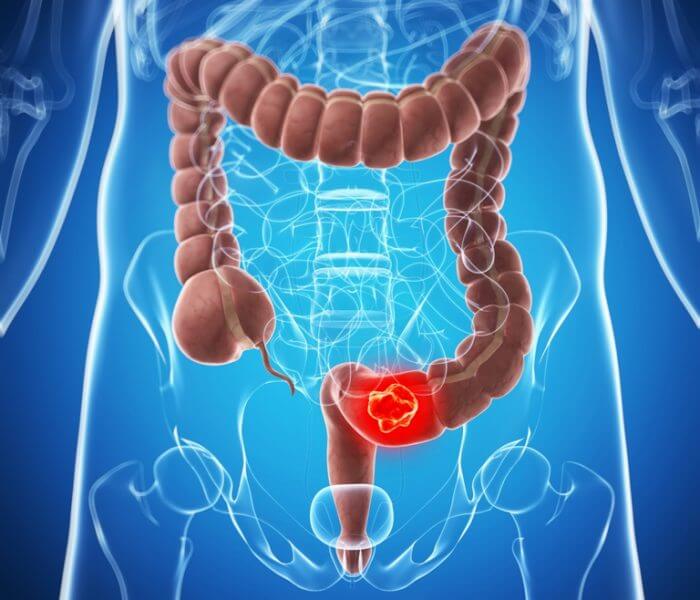
Typically, CRC is divided into colon cancer (in the large intestine) and rectal cancer (in the rectum). Treatment, prognosis and staging may differ depending on the exact site, tumour stage, and patient factors.
In Africa, as elsewhere, stage at diagnosis (how advanced the tumour is) remains a primary determinant of prognosis. The World Health Organization (WHO) notes that early diagnosis is a key step to improving outcomes.
Incidence in Africa
Recent research shows that the incidence of colorectal cancer in Africa is higher than earlier data suggested. A 2024 systematic review found age-standardised incidence rates (ASIR) for CRC of approximately 7.51 per 100,000 person-years in males and 6.22 in females.
Another 2022-based study estimated the continent’s incidence rate at 8.2 per 100,000 and mortality at 5.6 per 100,000. It also projected new cases to increase to ~168,683 by 2050 (from ~70,428 in 2022) if current trends persist.
Regionally, northern Africa shows higher incidence compared to western and southern regions; for example, ASIR in North Africa was estimated at ~9.66 per 100,000 for men.
Thus, although Africa’s overall incidence remains lower than many high-income regions, the trend is upward and burden will increase substantially without intervention.
Risk factors
Risk factors for colon/rectal cancer may be classified as non-modifiable and modifiable.
Non-modifiable risk factors:
- Age: although CRC is traditionally a disease of older adults, several African studies report a rising incidence among younger age groups (under 40) on the continent.
- Family history of colorectal cancer, genetic syndromes such as Lynch syndrome and Familial adenomatous polyposis (though data in Africa are less robust).
- Inflammatory bowel disease (e.g., ulcerative colitis, Crohn’s disease).
Modifiable risk factors:
- Diet: consumption of red and processed meats, butter, alcohol, and low fibre intake have been associated with increased risk in African data.
- Tobacco smoking.
- Obesity, physical inactivity.
- Urbanisation, changes in lifestyle and diet (the so-called ‘westernisation’ of diet) have been implicated in rising incidence across Africa.
In some African populations the traditionally high-fibre diet may have been protective but is being eroded by increased consumption of refined grains and ultra-processed foods.
Early signs and symptoms

Early colorectal cancer is often asymptomatic or causes non-specific symptoms. A key challenge in Africa is that when symptoms do appear they are often misattributed or ignored until advanced disease. For instance, the Cancer Association of South Africa (CANSA) notes that “in its early stages shows no symptoms. It is often diagnosed late when at a more advanced stage or it has spread.”
Common symptoms include:
- Change in bowel habits (e.g., persistent diarrhoea or constipation, change in stool consistency)
- Blood in stool or rectal bleeding
- Persistent abdominal discomfort (cramps, gas, pain)
- Feeling that the bowel does not empty completely
- Unexplained weight loss, fatigue
These symptoms, however, may also stem from benign conditions (e.g., haemorrhoids, infection), which can delay further investigation
Given the silent nature of early disease, awareness among patients and health-care workers is critical.
Early detection and screening
Early detection improves the chance of cure and reduces cost and morbidity. Screening aims to find disease (or pre-disease) in asymptomatic individuals. The WHO emphasises this component of cancer control.
In high-income countries screening is often by colonoscopy, faecal immunochemical test (FIT) or faecal occult blood test (FOBT). In Africa, however, screening programmes are scarce and face multiple barriers. A review of screening in Africa identified key impediments: limited endoscopic capacity (lack of colonoscopy infrastructure), low awareness among patients and providers, cultural/socio-demographic factors, cost and follow-up challenges.
Screening programmes that use simple, low-cost tests such as FIT may offer a practical pathway in resource-limited settings; but follow-up colonoscopy capacity must exist to complete the screening pathway.
One South African example: CANSA offers at-home stool tests for occult blood and refers positive cases for colonoscopy.
In summary, early detection in Africa remains significantly under-developed.
Prevention
Preventive strategies fall into primary (reducing risk before disease) and secondary (detecting disease early) prevention.
Primary prevention:
- Promoting healthy diet (high fibre, low processed meats, reduced red meat intake)
- Maintaining healthy body weight, engaging in regular physical activity
- Reducing alcohol consumption and smoking
- Encouraging awareness of family history and genetic risk
Several African dietary studies suggest that the traditional high-fibre diets may have been protective; shifting diets toward ultra-processed foods is increasing risk.
Secondary prevention:
- Implementing screening programmes in appropriate age/risk groups
- Training health-care workers to recognise early signs, refer appropriately
- Strengthening health infrastructure to allow timely diagnosis and treatment
Treatment
Treatment for colon/rectal cancer in Africa follows the same principles used globally: surgery, chemotherapy, radiotherapy (especially for rectal cancer), targeted therapies in selected cases, and palliative care when curative treatment is not feasible. The specific choice depends on tumour stage, patient performance status, comorbidities and resource availability.
However, the capacity to deliver optimal treatment is limited in many parts of Africa: fewer specialised cancer centres, lack of radiotherapy facilities in some regions, delays in surgery/chemotherapy, and limited access to newer targeted agents. As the American Cancer Society notes, for sub-Saharan Africa the five-year relative survival rate for CRC was estimated at ~31%—much lower than in high-income countries.
Delays in diagnosis, treatment initiation, and inadequate follow-up all contribute to poorer outcomes.
Prognosis
Prognosis depends on stage at diagnosis, tumour biology, patient health status and availability of treatment. In Africa, survival rates are markedly lower than in many Western countries due to the factors described above. For example, the ~31% five-year survival figure for CRC in low-HDI sub-Saharan settings is considerably lower than many high-income contexts.
Improving early detection, expanding screening participation, strengthening treatment capacity and reducing delays could improve outcomes.
Colon/rectal cancer is an increasingly important health issue across Africa. Incidence is rising, and the disease is expected to impose a growing burden unless preventive, detection and treatment systems are strengthened. Key actionable areas include raising awareness among both health-care workers and the public, improving access to screening (especially low-cost tests like FIT), expanding diagnostic and treatment infrastructure, and promoting lifestyle changes that reduce risk. While many of the challenges are substantial, progress in these domains could materially improve prognosis and reduce the human and economic toll of CRC across African countries.
Another preventable Cancer that burdens Africa is Cervical cancer, read here.
Frequently Asked Questions (FAQ)
Q: At what age should screening begin in Africa?
A: There are no widely adopted continent-wide guidelines for CRC screening in Africa. In some higher-resource settings and organisations such as CANSA in South Africa, screening (e.g., via stool test) is recommended around age 50 for average risk. (cansa.org.za) In countries with rising early-onset disease, clinicians may consider earlier discussion of family history and risk.
Q: Can simply eating more fibre prevent colon cancer?
A: A high-fibre diet is associated with reduced risk of colorectal cancer, likely via mechanisms such as faster transit time, binding of bile acids, production of short-chain fatty acids by gut bacteria, and reduced inflammatory exposure. However, diet is only one component of risk; other factors such as genetics, smoking, alcohol, obesity and access to care also matter.
Q: What types of treatment are available in Africa?
A: Treatment options mirror global standards: surgery (most important for localized disease), chemotherapy, radiotherapy (esp for rectal cancer), and in some centres targeted therapies or immunotherapy for selected patients. However, availability varies widely by country and region. Many patients face delays or limited access to these services.
Q: Why is the prognosis worse in African settings?
A: Multiple factors contribute: late-stage diagnosis, limited screening and early detection, inadequate infrastructure and specialist care, financial and geographic access barriers, and lower health-system capacity. Even when stage is similar, outcomes are worse in low-HDI countries.
Q: What are the most important steps a clinician in Africa can take?
A: Key steps include: maintaining a high index of suspicion for colorectal cancer when patients present with red-flag symptoms (e.g., rectal bleeding, persistent change in bowel habits), practising or referring for timely diagnosis (colonoscopy/biopsy), advocating for patient education about bowel cancer risk and screening, and collaborating with health-care systems to improve access to diagnostic and therapeutic services.
** This Article has been Reviewed by Dr. Chimaobi Felix, MBBS
⚕ Medical Disclaimer
This article is for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before making any health decisions. The Healthy African is not liable for any actions taken based on the information provided on this site.