By Dr Chukwunyere Chimaobi | Verified June 2026 | Sources: WHO, UNODC, The Lancet, PubMed, PLOS
A 28-year-old woman walks into a busy clinic in Lagos with three days of fever, headache, and aching muscles. Her doctor suspects malaria, prescribes artemisinin-based tablets, and sends her home. Two weeks later she returns, more unwell than before, with a rising temperature, abdominal pain, and a faint rash on her torso. She had typhoid fever all along. This kind of missed diagnosis happens across clinics in Nigeria, Ghana, Kenya, and beyond, more often than most people realise.

Malaria and typhoid fever are among the most common causes of fever in sub-Saharan Africa. They share enough symptoms to confuse both patients and health workers, particularly in settings where laboratory tests are not always available. Yet the two diseases are caused by entirely different organisms, spread through entirely different routes, and require entirely different treatments. Getting one confused for the other does not merely delay recovery; it can be fatal.
This article walks through the key differences between typhoid fever and malaria: how each disease begins, what symptoms to watch for, how doctors confirm which infection you have, and why treatment is not interchangeable.
Why these two diseases are so often confused
Both malaria and typhoid fever cause fever, headache, fatigue, and a general sense of being unwell. In many African clinics facing high patient loads and limited diagnostic support, treatment is sometimes prescribed on the basis of symptoms alone, a practice known as empirical treatment. The Africa Centres for Disease Control and Prevention (Africa CDC) notes that malaria remains the leading cause of febrile illness across much of sub-Saharan Africa, while typhoid fever is also widely endemic, particularly where sanitation is poor and clean water unreliable. When two such common illnesses look alike in their early stages, the risk of misdiagnosis is real and consequential.
What actually causes each disease
Malaria is caused by Plasmodium parasites, most commonly Plasmodium falciparum in Africa, and is transmitted through the bite of an infected female Anopheles mosquito. It cannot pass from person to person through casual contact.
Typhoid fever is a bacterial infection caused by Salmonella enterica serotype Typhi. It spreads through the faecal-oral route, meaning contaminated food or water. Poor sanitation, open defaecation, and unclean water sources are its main drivers in African communities.
This distinction already points to different prevention strategies: sleeping under an insecticide-treated mosquito net guards against malaria; drinking treated or boiled water and washing hands carefully before eating reduce the risk of typhoid.
How the symptoms differ
The character of the fever and its accompanying signs differ in ways a trained clinician, or an attentive patient, can learn to recognise.
Malaria tends to strike suddenly. The classic pattern is a cycle of cold chills and shivering (known as rigors), followed by a sharp temperature spike, heavy sweating, and a brief period of relative ease before the cycle repeats, typically every 48 to 72 hours depending on the parasite species. Nausea, vomiting, muscle pain, and headache are common. Severe malaria caused by P. falciparum can progress rapidly to cerebral malaria (infection affecting the brain), severe anaemia, or organ failure, sometimes within 24 to 48 hours.
Typhoid fever follows a different course. The temperature rises gradually over several days in a pattern clinicians call “stepladder fever,” climbing a little higher each day. By the end of the first week, the typical features include:
- A sustained high temperature, often 39-40°C, typically worse in the evenings
- A dull, persistent headache, rather than the throbbing headache more typical of malaria
- Abdominal pain and tenderness, particularly around the centre of the abdomen
- Constipation in the early stages, which may shift to diarrhoea as the illness progresses
- Relative bradycardia: the pulse is slower than would normally be expected for that level of fever, a subtle but useful clinical sign
- Rose spots: faint, salmon-coloured spots on the abdomen and chest, seen in a minority of patients but specific to typhoid
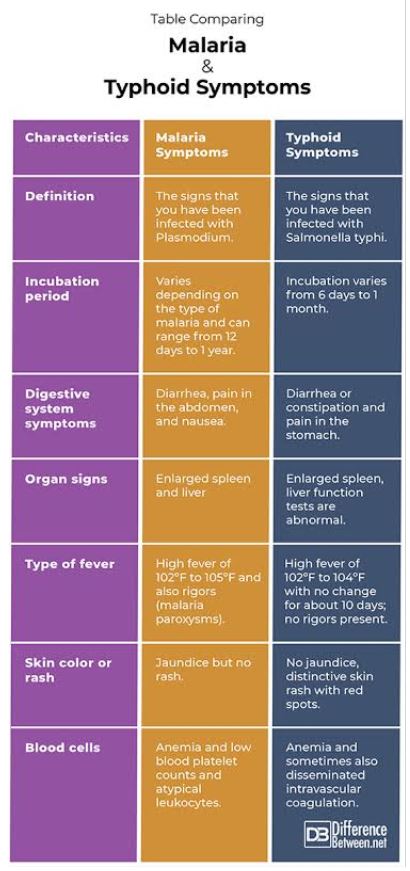
Rigors and profuse sweating, the hallmarks of malaria, are less typical in typhoid fever.
Diagnosis: why testing matters before treatment
In many African health facilities, the Widal test, a blood test that checks for antibodies against Salmonella Typhi, is commonly used to diagnose typhoid. The World Health Organization (WHO) advises caution with this test, however, because it has poor specificity and frequently produces false positive results in areas with previous typhoid exposure or high vaccination rates. Blood culture remains the gold standard for confirming typhoid, though it requires 48 to 72 hours and laboratory capacity that is not available at every primary care facility.
For malaria, a rapid diagnostic test (RDT) or microscopy using a thick and thin blood film provides a reliable same-day result. The WHO’s 2024 World Malaria Report (verified June 2026) emphasises that parasitological confirmation before treatment is essential, since treating based on fever alone risks overuse of antimalarials and contributes to drug resistance. Both categories of test are available at most secondary-level health facilities in Nigeria and across much of West and East Africa.
Treatment: one will not substitute for the other
Artemisinin-based combination therapies (ACTs), such as artemether-lumefantrine or artesunate-amodiaquine, are the first-line treatment for uncomplicated malaria, as recommended by the WHO and the Nigeria Centre for Disease Control and Prevention (NCDC). These drugs have no effect on bacterial infections such as typhoid fever.
Typhoid fever is treated with antibiotics. Azithromycin is currently recommended as first-line therapy for uncomplicated typhoid in many African settings, because of growing resistance to fluoroquinolones such as ciprofloxacin. Severe typhoid typically requires intravenous (IV) ceftriaxone and hospital admission.
Taking antimalarials when you have typhoid will not slow the bacterial infection. Taking antibiotics when you have malaria will not eliminate the parasite. This is why confirming the correct diagnosis before starting treatment, wherever testing is accessible, matters so much. If you are unsure about your diagnosis or are not improving on current treatment, speak to a qualified health professional before continuing or changing any medication.
When both infections occur at the same time
Co-infection, meaning having malaria and typhoid simultaneously, is not rare in sub-Saharan Africa. Published research, including studies in PLOS Medicine, has documented concurrent infections in children and adults in highly endemic areas where both diseases overlap. Patients with co-infection often present with a more severe illness and a clinical picture that is harder to interpret. If your symptoms do not improve as expected after treatment for one condition, ask your doctor whether both may be present and request testing for the other.
Frequently asked questions
Can you have typhoid and malaria at the same time? Yes, co-infection is documented and not unusual in parts of sub-Saharan Africa where both diseases are endemic. The illness tends to be more severe when both are present, and each infection must be treated separately. If you are not recovering as expected, tell your doctor and ask about testing for the other condition.
Is the Widal test a reliable way to diagnose typhoid fever? The Widal test is widely used across Africa but has well-known limitations. It can produce false positive results, particularly in areas where typhoid is common or where people have been previously exposed or vaccinated. Blood culture is more accurate, though less readily available at the primary care level. If you have a positive Widal result but are not improving on antibiotics, discuss further testing with your doctor.
How quickly can each disease become serious? Malaria caused by P. falciparum can become severe within 24 to 48 hours, particularly in children, pregnant women, and people with no prior malaria exposure. Typhoid worsens more gradually, over one to three weeks, but complications such as intestinal perforation or internal bleeding are life-threatening if the disease is left untreated.
What are the main ways to prevent each disease? Malaria prevention focuses on reducing mosquito exposure: sleep under insecticide-treated nets, use repellents, and remove standing water near your home. Typhoid prevention centres on safe water and sanitation: drink treated or boiled water, wash hands thoroughly before eating, and consider the typhoid vaccination, which is available at many clinics in Nigeria, Ghana, and Kenya.
Should I always get tested before taking malaria drugs? Yes, whenever testing is accessible. The WHO and most national treatment guidelines recommend parasitological confirmation before starting antimalarials. Treating without a confirmed diagnosis wastes medication, risks side effects, and may delay treatment for the actual cause of your illness.
Both malaria and typhoid fever are treatable when caught early and managed correctly. The single most important step you can take is to seek a confirmed diagnosis rather than self-medicate or rely on a previous prescription. If you or someone in your care develops a persistent fever, visit a clinic, request the appropriate test, and follow the treatment a qualified health professional recommends based on what the results actually show.
For a detailed look at malaria prevention, symptoms, and first-line treatment options available in Africa, see our earlier guide on malaria in Nigeria, to learn about antimalaria resistance read here.
This article draws on peer-reviewed and institutional sources including the WHO Africa Regional Office, UNODC World Drug Reports 2024 and 2025, The Lancet (2024), PLOS Global Public Health (2024, 2025), Frontiers in Public Health (2025), the Nigerian Medical Journal (2024), the Journal of West African College of Surgeons (2024), BMC Psychology (2025), and StatPearls/NCBI. All facts were verified in June 2026
** This Article has been Reviewed by Dr. Chimaobi Felix, MBBS
⚕ Medical Disclaimer
This article is for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before making any health decisions. The Healthy African is not liable for any actions taken based on the information provided on this site.